Accenture estimates that AI applications could save the global healthcare industry up to USD 150 billion annually by 2026, with patient experience among the highest-leverage use cases. Picture walking into a hospital where an AI co-pilot has already digested your medical history, surfaced your active medications, and pre-staged a personalized plan before you meet the clinician. That experience is no longer science fiction — it is being shipped today in leading U.S. health systems and European hospital networks alike.
At Agnotic Technologies we partner with hospitals, payers, and digital health startups across the U.S., U.K., Netherlands, and the Nordics to build AI-powered patient experiences that respect HIPAA, GDPR, and emerging European Health Data Space rules. This guide walks through the seven AI use cases reshaping patient experience in 2026 and how to operationalize them safely.
Understanding Generational Differences in Patient Experience
Patient expectations vary sharply across generations. Research from NRC Health and Deloitte highlights three persistent divides: how patients access information, how they share feedback, and how they evaluate quality of care.
Younger patients — Gen Z and millennials — favor smartphones, in-app messaging, and social media for health information. More than 70% of them research providers online before a first appointment, compared with fewer than half of baby boomers. They are far more likely to leave a review than respond to a paper survey, and they rank respectful communication and digital convenience above almost everything else. Older patients still prioritize clinical competency, continuity, and in-person reassurance.
Smart healthcare organizations meet patients where they are. Health systems we work with route Gen Z patients to in-app review prompts and short SMS surveys while sending older cohorts paper surveys with QR-code shortcuts back to a digital form. AI is what makes that segmentation feasible at scale.
Building Patient Experience Profiles
Personalized care begins with rich profiles. Leading systems aggregate clinical, behavioral, and patient experience data into role-specific summaries — one view for the front desk, another for the nurse, another for the attending. Done poorly, these profiles overwhelm staff. Done well, they sharpen every interaction.
AI co-pilots like NRC Health's Huey, Epic's MyChart Bedrock, and Microsoft Dragon Copilot synthesize records into concise insights. A clinician sees, for example, that a patient previously reported feeling dismissed and that taking ten extra seconds to acknowledge their concern correlates with substantially higher satisfaction scores.
Profiles only work when the underlying data flows in. That means closing the loop from intake forms, post-visit surveys, wearables, and digital therapeutics into a HIPAA-aligned, GDPR-respecting data platform — exactly the kind of infrastructure our Healthcare Data Engineering team builds for clients.
How AI Enhances Patient Experience
Across our engagements, seven AI patterns consistently move patient experience scores, operational efficiency, and clinical outcomes at the same time.
1. Predictive Analytics in Patient Care
Predictive analytics forecast outcomes, surface at-risk patients, and prompt proactive care. Readmission prediction, sepsis early warning, deterioration detection, and chronic-disease risk stratification all share the same blueprint — a HIPAA-aligned data pipeline, an interpretable model, and a workflow that lands the insight in front of the right clinician at the right time.
Predictive models also personalize surveys: ask the most relevant questions at the moment when the patient is most likely to engage. Response rates climb, signal-to-noise improves, and operational decisions sharpen.
2. AI-Enhanced Survey Development
Static surveys are giving way to dynamic ones. AI tailors question order, wording, and length based on the patient's responses and historic data. Patients see fewer redundant questions; researchers get richer answers; clinicians get insight that maps directly to actions they can take.
3. Personalized Outreach with AI
Generic reminders are noise. AI lets health systems send the right message — appointment, medication, vaccine prompt, mental-health check-in — through the right channel at the right time. Personalized outreach drives demonstrable lifts in adherence, no-show reduction, and patient-reported satisfaction.
4. Service Recovery with AI
Sentiment models scan written feedback, call-center transcripts, and public reviews to flag dissatisfied patients in near real time. A small service-recovery team can intervene within hours instead of weeks, turning detractors into loyal patients and protecting the system's reputation.
5. AI-Assisted Patient Scheduling
AI-assisted scheduling balances clinician utilization, patient preference, and clinical priority. The result is shorter wait times, less double-booking pain, fewer no-shows, and happier patients. Virtual health assistants surface the right appointment slots, answer routine questions, and free human schedulers to handle complex cases.
6. Enhanced Accuracy and Speed with AI
AI imaging and clinical decision support speed diagnosis without replacing clinicians. Tools from Aidoc, Rad AI, Google DeepMind, and IBM Watson Health are now embedded in production radiology and pathology workflows. Peer-reviewed studies — including landmark work published in Nature — show AI-augmented mammography reducing both false positives and false negatives in breast-cancer detection.
7. Empowering Proactive Health Management with AI
Wearables and home monitors stream vital signs, activity, and sleep data into AI models that detect deterioration early. PeraHealth's Rothman Index combines EHR signals into a live risk score; Yale-New Haven Health has reported a 29% reduction in sepsis mortality, and the Shannon Skilled Nursing Facility has reported a 14% drop in readmissions, after deploying it.
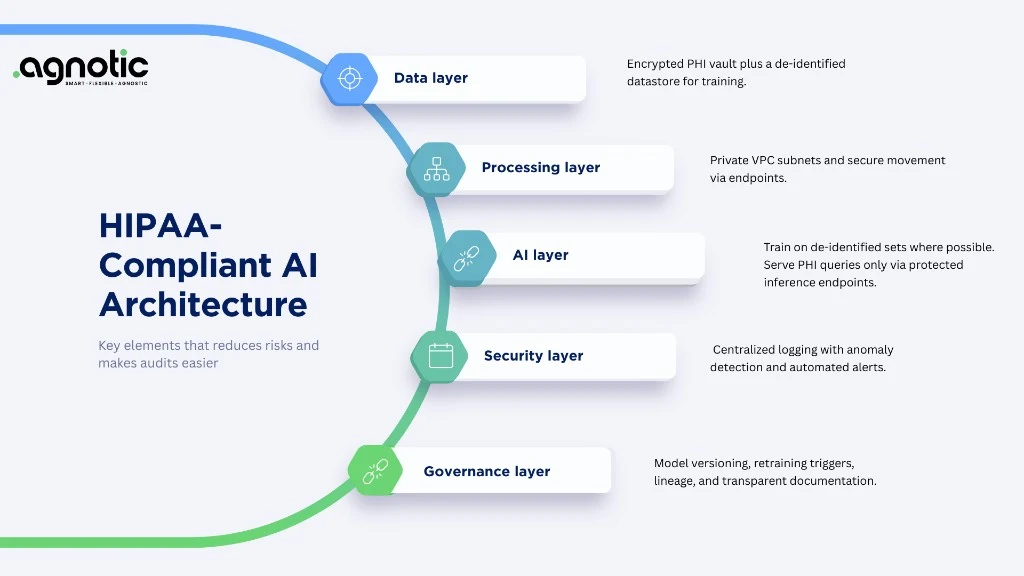
Operational Reality: Make It HIPAA- and GDPR-Safe
Every AI use case in this guide depends on patient data. That means HIPAA Business Associate Agreements with every subprocessor, GDPR Data Processing Agreements for EU data, secure prompt logging for any LLM in the loop, and strong access controls everywhere. None of this is optional, and shortcuts here jeopardize the rest of the program.
Our Healthcare Cloud & DevOps team builds the runways that make these AI workloads safe to operate at hospital and payer scale — from HIPAA-eligible landing zones on AWS, Azure, and GCP to confidential computing patterns for the most sensitive workflows.
Detailed Use Case Playbooks
1. Readmission Risk and Discharge Planning
Models trained on inpatient stays, social determinants of health, prior utilization, and post-discharge follow-ups can flag patients at risk of 30-day readmission. The intervention is what moves the needle: targeted post-discharge calls, pharmacist medication reconciliation, transportation support, and home-health visits. Health systems using mature workflows have reported 10-25% reductions in 30-day readmissions for targeted cohorts.
2. Sepsis and Deterioration Early Warning
Real-time models that combine vitals, labs, and EHR signals — PeraHealth's Rothman Index, Epic Sepsis, Google's MedLM-derived alerts — escalate clinical concern earlier. Treat these as decision support, not decision making: surface the alert, route to a rapid response team, and require clinician acknowledgement.
3. Ambient Clinical Documentation
Tools like Microsoft Dragon Copilot, Abridge, DeepScribe, Nuance DAX Copilot, and Suki listen to clinician-patient conversations and draft notes. The most consistent value lands as recovered clinician time (often 1-2 hours per shift) and reduced documentation burden. Implementation must address consent, BAA coverage, language localization, and EHR integration.
4. AI Scheduling and Demand Forecasting
AI-assisted scheduling combines patient preferences, clinician availability, no-show prediction, and demand forecasting. Pair the model with a 'wait list' or 'fill the gap' workflow that automatically pulls candidate patients into newly freed slots. Mature programs report 5-15% lifts in clinician utilisation and meaningful no-show reductions.
5. Patient Self-Service Virtual Assistants
Conversational assistants — built on Anthropic Claude, OpenAI on Azure, Google Gemini via Vertex AI, or AWS Bedrock — handle appointment reminders, prescription refill questions, and symptom triage. Anchor the assistant to retrieval-augmented generation grounded in approved sources, log every interaction, and route uncertain cases to a clinician quickly.
6. Sentiment-Driven Service Recovery
Sentiment models score patient feedback and public reviews in near real time. Set thresholds to alert a service-recovery team, escalate clinical safety concerns separately, and feed positive comments back to staff for reinforcement. Done well, this reduces detractors and surfaces systemic friction earlier than traditional survey programmes.
7. Imaging AI and Diagnostic Decision Support
AI imaging is already embedded in production radiology, pathology, and ophthalmology workflows. Tools from Aidoc, Rad AI, Annalise.ai, Gleamer, Lunit, and Paige integrate with PACS, EHR, and reporting systems. Plan for FDA 510(k) or CE marking, quality assurance protocols, and clinical change management — the technology is the easier half.
ROI Framework: What to Measure
Tie every AI patient-experience initiative to two or three KPIs that finance, operations, and clinical leadership all care about. The list below has been validated across U.S. health systems, EU integrated providers, and digital health startups.
- Patient satisfaction: HCAHPS, NPS, post-encounter pulse surveys, online review volume and sentiment.
- Operational efficiency: clinician minutes per encounter, documentation time, schedule fill rate, no-show rate.
- Clinical quality: readmission rate, sepsis mortality, length of stay, medication-error rate.
- Financial: revenue per encounter, write-offs, days in AR, denial rate, cost per acquisition for digital channels.
- Equity: subgroup performance gap on each of the metrics above, surfaced in monthly review.
- Trust: opt-in rate to AI-assisted features, drop-off rate during AI-mediated workflows, complaints per active user.
90-Day Implementation Roadmap
AI patient-experience programs land most reliably when they are scoped tightly, sequenced clearly, and tied to clinical and operational owners. The roadmap below maps to our standard engagement structure.
Days 1-30: Foundation
- Stand up the executive sponsor pair (clinical leader + operational leader).
- Pick one high-impact use case and define the success metrics with finance, clinical, and operations leadership.
- Document the data flow, HIPAA/GDPR posture, and BAA/DPA coverage for every component.
- Form a cross-functional squad: clinician, engineer, product, design, data, security, change management.
Days 31-60: Build and Validate
- Implement the MVP end-to-end, including monitoring, prompt logging, and rollback mechanisms.
- Run a clinical safety review and a security review before any live deployment.
- Pilot with a defined patient cohort and clinician group. Capture both quantitative and qualitative feedback.
- Tune the model, the UI, and the workflow until satisfaction and clinical comfort meet the bar.
Days 61-90: Scale and Operationalize
- Expand to additional service lines or sites with clear rollback criteria.
- Set up monthly KPI reviews and quarterly model performance audits.
- Train clinicians and staff on the new workflow; embed training into onboarding.
- Plan the next use case based on what the first one taught you.
Vendor Ecosystem Worth Evaluating
- Patient feedback and experience analytics: NRC Health, Press Ganey, Qualtrics XM Health, Feedtrail, Glassbox.
- Conversational AI and patient self-service: Hyro, Notable, Soul Machines, Conversa Health, Smart Robin, Babylon.
- Ambient documentation: Microsoft Dragon Copilot, Abridge, DeepScribe, Augmedix, Suki, Nabla.
- Imaging AI: Aidoc, Rad AI, Annalise.ai, Gleamer, Lunit, Paige, Tempus.
- Predictive analytics: Jvion, KenSci, Epic Cognitive Computing, Health Catalyst, Closedloop.ai.
- Scheduling and operations: LeanTaaS, Qventus, Olive, Notable, Hospital IQ.
- Patient outreach: Twistle, Luma Health, Relatient, Phreesia, mPulse Mobile.
- Data platforms: Snowflake Healthcare, Databricks Lakehouse for Healthcare, Google Healthcare Data Engine, AWS HealthLake, Azure Health Data Services.
Change Management Patterns That Work
Technology is only the front end of the work. The teams that ship AI patient experience successfully invest in change management with the same rigour they invest in engineering.
- Lead with clinicians and patient advocates, not vendors. Their early endorsement carries the program.
- Build a 'champion network' — early adopters who help train peers, surface problems, and translate AI into clinical context.
- Communicate honestly about what the AI can and cannot do. Surprises erode trust faster than known limitations.
- Time training to coincide with deployment, not weeks before; reinforcement matters more than upfront instruction.
- Make it easy to opt out. Patients and clinicians who feel coerced into AI workflows churn quickly.
- Celebrate wins publicly, share failures privately, and learn from both.
Pitfalls We See on Patient-Experience AI Programs
- Trying to do everything at once. Pick a use case, ship it, learn, then expand.
- Treating LLMs as decision makers. They are excellent collaborators and dangerous deciders.
- Skipping subgroup performance reviews. Equity gaps that go unmeasured grow.
- Underinvesting in clinician change management. Models without adoption are shelfware.
- Forgetting language coverage. Multilingual patients are often the highest-leverage group; serve them first.
- Centralising data without a clear governance model. A data lake without rules is an audit finding waiting to happen.
Authoritative References
- Accenture — AI in Healthcare
- U.S. ONC — Healthcare AI Resources
- EU — European Health Data Space
- NHS England — AI Lab
- WHO — Ethics & Governance of AI for Health
Conclusion
AI is reshaping patient experience in measurable ways. Predictive analytics, dynamic surveys, personalized outreach, service recovery, AI scheduling, AI-augmented diagnostics, and connected wearables — each pattern, deployed well, lifts patient satisfaction, clinician productivity, and clinical outcomes simultaneously. The remaining work is operational: pipe the right data into the right model behind the right safeguards, then close the loop with clinicians and patients. Agnotic Technologies builds and runs those systems with healthcare leaders across the U.S. and EU.