In 2018, IBM's Watson for Oncology became a cautionary tale when investigators reported that the system had recommended unsafe cancer treatments. Eight years later, the question is no longer whether AI belongs in HealthTech — it does — but how to deploy it responsibly across the United States, the United Kingdom, and the European Union, where regulators, payers, and patients are all watching.
From AI-assisted diagnostics and remote monitoring to genomics platforms and digital therapeutics, the technology stack is expanding faster than the ethical guardrails around it. At Agnotic Technologies, we build healthcare products that move quickly without losing sight of the values that make medicine trustworthy. This guide walks through the ethical issues every HealthTech leader should plan for and the professional standards that turn those plans into practice.
Why HealthTech Ethics Matter Now
Health technology produces immediate, life-altering outcomes. A misclassified lesion, a biased risk score, or a leaked diagnosis can change a patient's care, employment, and insurance. The regulators who oversee the field have responded: the U.S. FDA continues to refine its Software as a Medical Device (SaMD) framework, the European Medicines Agency works alongside national competent authorities under the MDR/IVDR, and the EU AI Act now classifies most clinical AI as high-risk.
Ethics is not a brake on innovation. It is the operating system that allows innovation to scale into hospitals, payers, and consumer markets that demand both speed and accountability.
Core Ethical Issues in HealthTech
Modern health technology raises a recurring set of ethical questions. Each is distinct, but together they form the matrix that founders, product leaders, and engineers must navigate.
Equity and Access
Wearables, remote patient monitoring kits, and AI-powered diagnostic tools tend to reach affluent, well-insured populations first. Without intentional design, HealthTech can deepen rural-urban divides in the U.S., widen North-South gaps in the EU, and amplify the digital exclusion already documented in NHS England's Core20PLUS5 framework.
Equitable HealthTech designs for the slowest network, the cheapest device, and the most underserved community first — then optimizes from there.
Algorithmic Bias and Discrimination
Diagnostic models trained on narrow datasets perform worse on under-represented groups. Pulse oximeters that under-read in darker skin tones, dermatology AI that misses melanoma in Black patients, and predictive risk tools that under-allocate care to minority cohorts are well-documented failure modes.
Mitigations include diverse training data, subgroup performance reporting, fairness audits aligned with the NIST AI Risk Management Framework, and ongoing post-market surveillance.
Privacy and Security
Health data is permanent. A leaked HIV status or genomic profile cannot be undone. HIPAA in the U.S., GDPR Article 9 and the EHDS Regulation in the EU, and the UK Data Protection Act combine to set a high bar — but compliance is the floor, not the ceiling. Build with privacy-by-design (Article 25 of GDPR) and use Privacy Enhancing Technologies where feasible.
Safety and Informed Consent
New tools introduce new risks. Patients deserve to understand the limits of an AI assistant, the failure modes of a wearable, and the data flows behind a digital therapeutic. Plain-language consent, accessible disclosures, and a clear escalation path to a clinician are non-negotiable.
Effectiveness and Clinical Evidence
Not every promising prototype earns a place in care. Rigorous evaluation — ideally through pre-registered clinical studies, real-world evidence, and post-market surveillance — separates HealthTech that helps from HealthTech that distracts.
Accountability and Responsibility
When a model recommends the wrong therapy, who is responsible? The clinician? The developer? The hospital? The EU AI Act, FDA Predetermined Change Control Plans, and emerging case law all push toward distributed accountability with clear contractual and technical guardrails.
How to Handle Ethical Issues in HealthTech
An ethics program is not a poster on the wall. It is a workflow that surfaces issues, routes them to qualified reviewers, and produces documented decisions. The most effective HealthTech teams we work with follow a five-step loop.
- Acknowledge and investigate: surface concerns through structured channels (engineering retros, clinical advisory boards, post-market reports) and treat anonymous reports with equal seriousness.
- Categorize the violation: is it a process gap, a policy gap, or a clinical risk? An action can be legal yet unethical — that is still a problem.
- Involve experts: convene an ethics committee that mixes clinicians, engineers, patients, and legal counsel before high-stakes decisions.
- Update policies: encode the lesson in your SDLC, training, and procurement processes so the same issue does not resurface.
- Train and audit: run regular workshops, refresh policies against the latest ACM, AMA, and AMIA guidance, and audit against your own commitments.
Essential Professional Standards for HealthTech
Standards turn principles into practice. The teams we partner with adopt these baselines:
- Clinical care standards: evidence-based design reviewed against the latest NICE, AHRQ, or specialty-society guidance.
- Patient-centered care: shared decision-making, accessibility (WCAG 2.2 AA, EN 301 549), and inclusive design.
- Safety standards: structured risk management aligned with ISO 14971 and IEC 62304.
- Ethical standards: explicit commitments to beneficence, autonomy, justice, and non-maleficence, with periodic third-party review.
- Continuing competence: required training, certification, and conference attendance for clinical and engineering staff.
- Documentation and record-keeping: tamper-evident audit logs, EHR-grade retention, and discoverable design history files.
- Collaboration and teamwork: multi-disciplinary squads, paired clinician-engineer design reviews, and frequent retrospectives.
- Resource utilization: pragmatic cost-of-care analysis baked into product reviews so HealthTech does not push price up while pushing outcomes only marginally forward.
- Patient and family education: micro-learning, in-app tutorials, and culturally appropriate explanatory content.
- Quality improvement: KPIs that include subgroup performance, patient-reported outcomes, and incident rates — reviewed monthly.
The Role of Regulation and Governance
Regulation is the backbone that holds ethics in place across competitors. In the U.S., the FDA's premarket pathways (510(k), De Novo, PMA) and the Office of National Coordinator's HTI-1 Rule shape what gets to market. In the EU, MDR, IVDR, GDPR, the AI Act, and the upcoming European Health Data Space create one of the most comprehensive frameworks in the world. The U.K. MHRA, Health Canada, Australia's TGA, and Singapore's HSA add further checkpoints for global launches.
Professional codes — the AMA Code of Medical Ethics, the AMIA Code of Professional and Ethical Conduct, and the World Medical Association's Declaration of Helsinki — bind individual practitioners. Build your governance program so that organizational policies and individual codes reinforce each other rather than diverging under pressure.
Real-World Failures We Should Have Learned From
Concrete failures sharpen ethical instincts in a way that abstract principles never will. The cases below are widely cited in HealthTech ethics curricula and should inform every product decision you make.
IBM Watson for Oncology (2018)
Internal documents revealed Watson recommended unsafe and incorrect treatments — not because the model was malicious, but because training data was largely synthetic and reviewed by a narrow set of physicians at a single institution. The lesson: representative, multi-site clinical data matters more than model size.
The Optum/UnitedHealth Risk Score (2019)
An algorithm widely used by U.S. health systems systematically under-allocated care to Black patients because it used historical healthcare spend as a proxy for need. Black patients with the same risk level received fewer high-touch interventions than white patients. The fix required swapping the target variable for active chronic conditions and retraining — a reminder that proxy variables embed historic inequities.
Dermatology AI for Skin Cancer (2018-2023)
Multiple dermatology AI models were shown to miss melanoma on darker skin tones at significantly higher rates because their training data came overwhelmingly from light-skinned cohorts. Newer datasets such as the ISIC 2020 challenge and the Fitzpatrick 17k corpus exist precisely because of these failures, but many production models still ship without subgroup audits.
Pulse Oximetry Bias (Long-Standing, Reconfirmed 2020-2024)
Pulse oximeters over-report blood oxygen on darker skin tones, with documented clinical consequences during COVID-19 triage. The FDA's 2024 panel review is reshaping how SaMD pulse-ox features must validate accuracy across Fitzpatrick scales — a standard every wearables team should already be applying.
Predictive Sepsis Models (Epic Sepsis Model, 2021)
Independent validation in JAMA Internal Medicine showed that a widely deployed sepsis prediction model performed far worse in real-world settings than vendor claims suggested. The case highlights why post-market surveillance, prospective trials, and silent-mode deployments matter as much as initial accuracy reporting.
Algorithmic Bias: A Practical Playbook
Fairness is engineered, not declared. The teams we work with treat bias mitigation as a four-step loop and run it on every model that touches patient-facing decisions.
- Audit the inputs: characterize the training and validation data by age, sex, race or ethnicity, geography, payer mix, language, and clinical setting. Flag gaps before training begins.
- Audit the outputs: compute subgroup performance for sensitivity, specificity, PPV, NPV, calibration, and clinical utility. Publish the table internally before shipping.
- Mitigate where needed: rebalance training data, apply reweighting or adversarial debiasing, calibrate per subgroup, or restrict the model's intended use until performance gaps close.
- Monitor in production: track drift in performance by subgroup, surface alerts when calibration degrades, and feed real-world performance back into the next training cycle.
Frameworks to Anchor the Work
- NIST AI Risk Management Framework — playbook for trustworthy AI, including socio-technical risks.
- FDA Good Machine Learning Practice (GMLP) — 10 guiding principles co-authored with Health Canada and the U.K. MHRA.
- ISO/IEC 23894 — AI risk management standard.
- ISO/IEC TR 24028 — overview of trustworthiness in AI.
- U.K. NHS AI Lab Buyer's Guide — practical evaluation criteria for clinical AI.
Patient Consent and Transparency UX
Consent is where ethics meets product design. The strongest consent experiences combine plain-language explanations, layered disclosures, granular opt-ins, and a visible audit trail.
- Use a sixth-grade reading level for primary consent text and link out to detail.
- Separate the consent for treatment, the consent for data use, the consent for marketing, and the consent for AI processing.
- Translate consent into the patient's preferred language; do not lean on browser auto-translate.
- Surface withdrawal mechanisms inside the product — not buried in a help center.
- Log every consent decision with a timestamp, version of the policy, and the locale displayed.
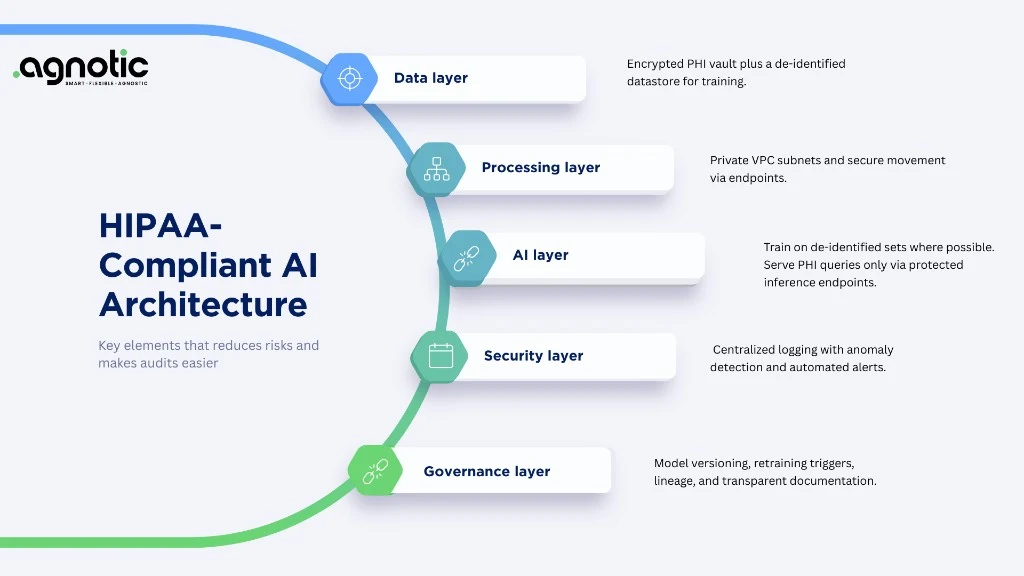
Governance Operating Model
Ethical commitments are durable only when they are wired into how the company operates. Start with three artifacts:
- An AI policy that names allowed use cases, banned use cases, and the review process for borderline ones.
- A model card and a data card for every production model. Update both when training data, performance, or scope changes.
- A risk register that maps each model to its harms, controls, and post-market surveillance plan.
Reinforce those artifacts with an Ethics Review Board, a clear escalation path for engineering and clinical staff, and a customer-facing channel for patients and clinicians to flag concerns. Boards work best when patient advocates and outside clinicians are paid for their time rather than volunteering.
EU AI Act Deep Dive: What Healthtech Founders Must Know
The EU AI Act (Regulation 2024/1689) entered into force in 2024 and most healthtech use cases land in the high-risk category under Annex III or because they constitute safety components of medical devices regulated under MDR/IVDR. The deadlines that matter most:
- Prohibited practices: applicable from February 2025. Examples include real-time biometric identification in public spaces and systems that exploit vulnerabilities of patients.
- General-purpose AI obligations: applicable from August 2025. Transparency, technical documentation, and copyright compliance for foundation-model providers.
- High-risk obligations: applicable from August 2026 for most systems, with extended timelines for embedded medical-device AI. Plan now for risk management, data governance, technical documentation, human oversight, accuracy/robustness/cybersecurity, and post-market monitoring.
- Fines: up to EUR 35 million or 7% of global annual turnover for prohibited practices, EUR 15 million or 3% for high-risk non-compliance.
Operationally, expect to publish technical documentation aligned with Annex IV, register your system in the EU database, and integrate AI Act obligations with your existing MDR/IVDR Quality Management System. Notified bodies are still ramping up; engage early and budget for review delays.
Building an Internal Ethics Function
Even a small startup can stand up a meaningful ethics function. Three pragmatic steps:
- Appoint an executive sponsor (often the CMO or CTO) who owns the ethics program at the leadership table.
- Form a cross-functional Ethics Review Board that meets monthly, with clinicians, engineers, designers, legal, and at least one external patient advocate.
- Publish quarterly transparency reports — even short internal ones — describing model performance, incidents, mitigations, and roadmap.
Metrics That Tell You the Program Is Working
- Subgroup performance gap (max difference in sensitivity or PPV across demographic strata).
- Time from incident report to triage decision.
- Patient-reported satisfaction across demographic strata.
- Number of clinical advisory board recommendations implemented vs deferred.
- Percentage of models with current model cards and post-market monitoring plans.
- Accessibility audit pass rate (WCAG 2.2 AA, EN 301 549).