Healthcare runs on data, but the more we centralize that data the more attractive it becomes to attackers — and the more difficult it becomes to comply with HIPAA in the United States, GDPR across the European Union, and the upcoming European Health Data Space (EHDS) regulation. Federated Learning (FL) and Quantum-Safe Cryptography (QSC) offer a different path: train powerful models and run rich analytics on patient data without that data ever leaving the institution where it was created.
At Agnotic Technologies we build privacy-preserving healthcare platforms for U.S. health systems, EU research consortia, and digital health startups in the U.K. and the Nordics. This guide explains how FL, QSC, and the open-source OpenFHE library combine to protect patient privacy while preserving the analytical value of clinical data.
1. The Challenge of Patient Data Protection
Hospitals, payers, and research networks need to share insights — not raw records. Yet most legacy pipelines still move data into a central lake, where it sits encrypted at rest but exposed at query time. Add the looming threat of cryptographically relevant quantum computers, and the cryptographic primitives that protect today's healthcare data will not protect tomorrow's.
2. Federated Learning in Healthcare
Federated Learning flips the script. Models travel to the data instead of the other way around. Each site trains locally on its EHR records, imaging studies, or genomic data; only aggregated model updates leave the perimeter. The result is a global model that has effectively learned from every participating cohort without violating any data residency, contractual, or regulatory boundary.
We see FL succeed most often in three patterns: cross-hospital diagnostic model training, multi-payer fraud detection, and federated digital pathology where image sizes make centralization impractical anyway.
3. What Is Quantum-Safe Cryptography?
Quantum-Safe Cryptography (also called Post-Quantum Cryptography, or PQC) refers to cryptographic algorithms believed to resist attacks from sufficiently powerful quantum computers. PQC schemes target the moment — likely a decade out, but possibly sooner — when Shor's algorithm running on a fault-tolerant quantum machine can break RSA, Diffie-Hellman, and elliptic-curve cryptography.
For healthcare data, the threat is not theoretical. "Harvest now, decrypt later" attacks assume adversaries are stockpiling encrypted health data today, ready to decrypt it once quantum capability matures. PQC is the answer.
4. Introducing OpenFHE
OpenFHE is an open-source library that combines efficient implementations of every major Fully Homomorphic Encryption (FHE) scheme. It builds on lessons from PALISADE, HElib, and HEAAN, and exposes a cross-platform API that healthcare engineering teams can wire into Python, C++, Rust, and Go pipelines.
What Is Homomorphic Encryption?
Homomorphic Encryption (HE) lets you compute directly on encrypted data. The output, when decrypted, equals what you would have gotten from running the same computation on the plaintext. HE makes it possible to outsource analytics to a third party — a cloud, a research collaborator, a payer — without ever exposing the underlying records.
Unlike Secure Multi-Party Computation, HE does not require multiple parties to cooperate at every step. A single entity holds the key and the rest of the world operates on ciphertexts. That property is invaluable for outsourced AI inference, secure model deployment, and protecting proprietary model weights when shipping into an untrusted environment.
Use cases extend beyond healthcare into smart grids, finance, education, and Machine Learning as a Service. They share one feature: input privacy is a hard requirement, and the computation cannot be trusted to a single tenant.
5. The NIST PQC Standardization Process
The U.S. National Institute of Standards and Technology runs the formal process that selects PQC algorithms for global use. The same standards are referenced by ENISA in the EU and by the U.K. National Cyber Security Centre.
Call for Submissions
NIST invited researchers worldwide to submit quantum-resistant algorithms. Dozens of academic teams, vendors, and national labs responded with candidates spanning lattice-based, code-based, hash-based, and isogeny-based mathematics.
Rounds One, Two, and Three
Each round narrowed the field through public cryptanalysis. After three rounds, NIST selected four algorithms for standardization: CRYSTALS-KYBER (key establishment), CRYSTALS-Dilithium (digital signatures), FALCON, and SPHINCS+.
Why These Four?
KYBER and Dilithium were chosen for their balance of security and performance. FALCON addresses use cases where Dilithium signatures are too large. SPHINCS+ provides a stateless hash-based fallback so that not every system relies on lattice security.
Round Four and Beyond
NIST continues to evaluate additional KEMs (BIKE, Classic McEliece, HQC, SIKE) to diversify the cryptographic backbone. Classic McEliece remains under consideration for archival use cases despite its large key size.
6. How FL and QSC Work Together
FL and QSC reinforce each other. The result is a stack that protects data in motion, at rest, and during computation — every state where patient records have historically been vulnerable.
- Privacy-preserving model aggregation: model updates travel encrypted with PQC algorithms, so even the aggregator cannot infer individual contributions.
- Homomorphic encryption for data privacy: when FL alone is not enough, HE allows computation on encrypted local data before aggregation.
- Quantum-resistant data transmission: every channel between sites uses post-quantum TLS profiles, mitigating harvest-now-decrypt-later risk.
- Quantum-resilient data fusion: cross-institution model fusion uses lattice-based KEMs so that long-lived ciphertexts remain protected.
- Privacy preservation by design: OpenFHE keeps patient data encrypted across the lifecycle of any analytic workload.
Regulatory Compliance Built In
Federated learning paired with quantum-safe cryptography maps cleanly onto HIPAA Technical Safeguards, GDPR Article 32, the upcoming EHDS Regulation, and ISO/IEC 27701. By keeping raw data on-premise and protecting model updates with PQC, healthcare organizations satisfy regulators on both sides of the Atlantic.
- Data security: cryptographic posture survives both classical and quantum attacks.
- Regulatory compliance: HIPAA, GDPR, EHDS, NHS DSPT, and PIPEDA controls map naturally onto OpenFHE-based workflows.
- Collaborative research: research consortia retain data sovereignty while contributing to multi-site studies.
7. Implementation Realities
Technical Implementation
Integrating OpenFHE into existing healthcare infrastructure is a deliberate engineering exercise. Our team typically starts with a containerized reference architecture, threat models the data flows, and stages the migration so that live workloads are never disrupted.
Computational Overhead
Homomorphic encryption is computationally expensive. Recent FHE schemes and GPU-accelerated implementations have narrowed the gap, and selective use of HE for the most sensitive workloads keeps overall costs manageable. Where FHE is too heavy, we combine FL with differential privacy and trusted execution environments.
8. Future Directions
- Advancements in quantum-safe cryptography: faster lattice-based schemes, hybrid TLS profiles, and standardized key exchange across the Internet.
- Optimized federated learning: improved convergence, secure aggregation, and reduced communication overhead.
- Wider adoption: as research consortia, payers, and hospital systems standardize on OpenFHE and PQC, expect a step-change in privacy-preserving collaborative care.
9. Hospital-Network Case Studies
Federated learning has moved from research papers into multi-site production. The examples below are widely cited in the industry and worth studying as you design your own architecture.
Owkin and BeiGene's Federated Oncology Network
Owkin operates federated learning across cancer centers in Europe and North America, training survival models, treatment response classifiers, and biomarker discovery models without raw patient data ever leaving each site. The result has been clinically meaningful improvements in stratification for trials and real-world outcomes research.
NVIDIA Clara FL
NVIDIA's Clara federated learning framework powers cross-institution collaborations in radiology, pathology, and genomics. Notable deployments include the EXAM model for COVID-19 oxygen-need prediction, trained across 20 hospitals on four continents in less than two weeks — without centralizing imaging data.
MELLODDY (Machine Learning Ledger Orchestration for Drug Discovery)
Ten of the world's largest pharmaceutical companies trained shared predictive models for drug discovery using federated learning while keeping their proprietary chemical libraries on-premise. MELLODDY proved that competitive entities can collaborate cryptographically — a lesson hospital networks and payers are now applying.
U.K. NHS AI Lab — National Medical Imaging Platform
The NHS AI Lab has piloted federated workflows for chest X-ray classification across NHS trusts. The platform combines on-site model training, central evaluation, and strict information governance review — a useful template for any national health system contemplating cross-trust collaboration.
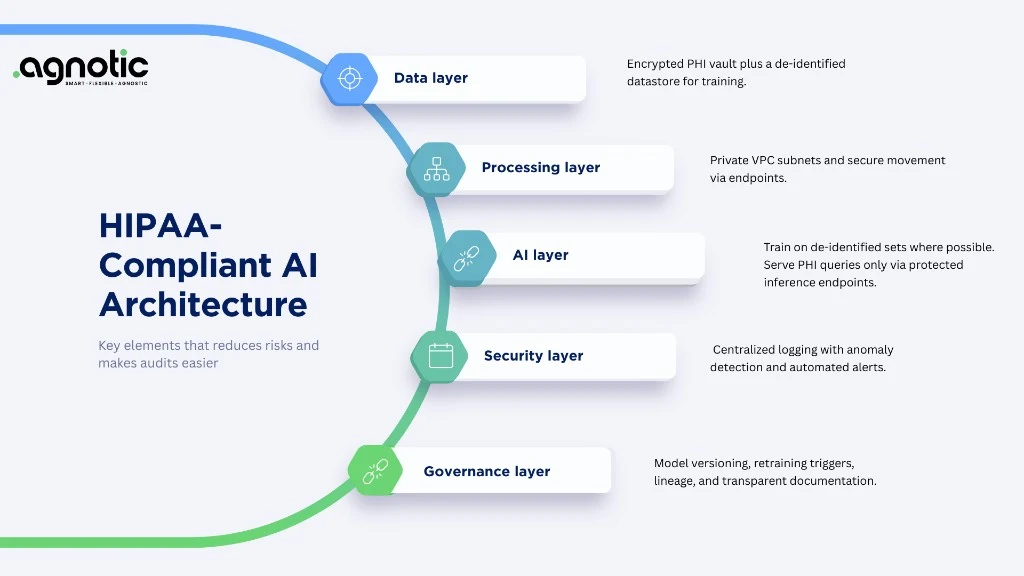
10. Reference Architecture for FL + PQC + OpenFHE
A production-grade federated learning platform with quantum-safe transport and selective homomorphic computation typically has the following layers.
- Edge runtime: each participating site runs a containerized FL client (commonly Flower, NVIDIA FLARE, OpenFL, or PySyft) inside their secure perimeter. Local data never leaves the site.
- Secure aggregation: the central aggregator combines encrypted model updates using secure aggregation protocols (e.g., Bonawitz et al.), differential privacy, and additional masking where required.
- Quantum-safe transport: every channel between client and aggregator uses hybrid TLS profiles combining classical curves with NIST-selected PQC primitives such as ML-KEM (Kyber).
- Selective FHE: highly sensitive aggregations (rare-disease counts, biomarker computations, multi-payer claims) execute under OpenFHE with BGV, BFV, or CKKS — chosen based on the workload's arithmetic profile.
- Identity and audit: site identities are anchored in PQC-signed certificates (Dilithium or FALCON), and every model update is logged in an append-only audit store reviewed by information governance committees.
- Model registry: a central registry tracks model lineage, training cohorts, performance by site, and post-market monitoring metrics — essential evidence for FDA pathways and EU MDR documentation.
11. OpenFHE Scheme Selection Guide
OpenFHE bundles several FHE schemes. Choosing the right one is the difference between an unusable prototype and a production-grade workload.
- BFV / BGV: integer arithmetic for tasks like federated counts, contingency tables, and survey aggregation. Strong throughput, predictable performance.
- CKKS: approximate arithmetic on real numbers — the right choice for federated machine learning over encrypted weights, secure neural-network inference, and risk-score aggregation.
- TFHE / FHEW: bit-level operations and arbitrary functions on encrypted booleans. Useful for secure decision trees and small lookup tables.
- Hybrid: combine FHE for the most sensitive sub-computation with secure aggregation for the rest. Almost every successful production deployment uses a hybrid approach.
12. Performance, Cost, and Hardware Acceleration
Concerns about FHE performance are dated. Several factors have closed the gap dramatically over the past two years:
- GPU acceleration: NVIDIA cuFHE, Microsoft EVA, and academic libraries deliver 10-100x speed-ups on lattice-based operations.
- Hardware acceleration: Intel HE Accelerator, IBM HElayers, and emerging FPGA designs cut FHE multiplications from seconds to milliseconds.
- Smarter scheme selection: applying CKKS only to the layers that need it (typically the final aggregation) keeps the rest of the workload at near-plaintext speed.
- Cloud confidential compute: AWS Nitro Enclaves, Azure Confidential VMs, and GCP Confidential Computing reduce the surface where FHE is strictly necessary.
On the cost side, expect FHE-protected federated training of a mid-sized clinical model to add 15-40% to compute cost relative to a centralized baseline — well within the budget envelope for regulated workloads.
13. A 6-Phase Implementation Roadmap
We typically sequence federated, quantum-safe healthcare projects across six phases. Timelines vary, but the structure holds for both single-payer hospital networks and pan-EU research consortia.
- Phase 1 — Charter and governance: define scope, participating sites, information governance approvals, and the model registry.
- Phase 2 — Cryptographic inventory: document every cryptographic dependency and identify the workloads that justify PQC and FHE adoption.
- Phase 3 — Pilot FL: run a non-clinical pilot (operational metrics, benign clinical signals) to validate plumbing without touching live patient care.
- Phase 4 — Add PQC transport: introduce hybrid TLS, PQC-signed site identities, and quantum-safe key management.
- Phase 5 — Selective FHE: identify one or two computations where FHE delivers disproportionate privacy value (rare disease counts, biomarker discovery) and deploy OpenFHE around them.
- Phase 6 — Operationalize: continuous validation, model drift monitoring, post-market surveillance, and integration with FDA or EU regulatory submissions.
14. Regulatory & Procurement Considerations
Regulators on both sides of the Atlantic increasingly expect quantum-safe migration planning even before final NIST standards are universally adopted.
- U.S. CISA, NSA, and NIST jointly published quantum-readiness guidance in 2023 and 2024 — federal contracts now ask about PQC roadmaps.
- U.K. NCSC published its PQC migration timeline in 2024, with key government workloads expected to use PQC by 2031.
- European Commission and ENISA are aligning PQC guidance with the NIS2 Directive and the upcoming Cyber Resilience Act.
- GDPR Article 32 already mandates 'state of the art' security — a defensible interpretation in 2026 increasingly includes quantum-safe transport for long-lived health data.
- HIPAA Security Rule modernization signals expectations around modern key management and inventories, which serve as natural foundations for PQC migration.
15. Common Pitfalls We See in the Field
- Underestimating the orchestration cost of federated learning. Most projects fail at the people layer, not the math.
- Using FHE everywhere instead of selectively. Performance budgets collapse; teams abandon the project.
- Skipping a cryptographic inventory before piloting PQC. Without an inventory you cannot prioritize the migration.
- Treating differential privacy as optional alongside FL. Without DP, model updates can still leak training samples.
- Forgetting information governance approvals. The strongest cryptography in the world cannot replace IG sign-off in U.K. and EU health systems.
- No post-market monitoring. Federated models drift; without monitoring, drift becomes invisible.
Conclusion
Privacy and progress are no longer at odds in healthcare. Federated Learning, Quantum-Safe Cryptography, and OpenFHE let providers, payers, and researchers collaborate at a global scale without leaking patient data — and without leaving long-lived records exposed to tomorrow's quantum threats. Agnotic Technologies helps teams design, build, and operate the resulting platforms across the U.S., U.K., and EU.